Most women who are diagnosed with polycystic ovary syndrome hear the name and walk away with more questions than answers. What is actually happening inside the body? Why does it affect so many different things at once, from periods to skin to weight to mood? And why do some doctors call it a hormonal condition while others call it a reproductive one?
The reason PCOS touches so many systems in the body is because it starts with hormones. Polycystic ovary syndrome is one of the most common hormonal conditions affecting women of reproductive age. It is estimated to affect between 1 in 5 and 1 in 10 women in India, though many go undiagnosed for years. Many women also explore treatments such as polycystic ovary syndrome electrolysis to manage excess facial and body hair caused by hormonal imbalances, alongside medical care that addresses the underlying condition.
This article explains what PCOS is, why it is classified as an endocrine disorder, how it develops in the body, and what women can do about specific symptoms like excess hair growth, including whether electrolysis is a suitable option.
What is Polycystic Ovary Syndrome?
Polycystic ovary syndrome is a condition where the ovaries do not function the way they should, because of an underlying imbalance in hormones.
The name can be misleading. Not every woman with PCOS has cysts on her ovaries. And some women who do have ovarian cysts do not have PCOS. The condition is diagnosed based on a set of criteria rather than a single finding.
Doctors typically look for two of the following three features to confirm a diagnosis:
- Irregular, infrequent, or absent menstrual periods
- Evidence of elevated male hormones, either through a blood test or through symptoms such as excess hair or acne
- Polycystic-appearing ovaries on an ultrasound scan, where multiple small follicles are visible
Polycystic ovary syndrome is a lifelong condition. It does not go away on its own. But with the right management, most women can control their symptoms effectively and live well.
Is PCOS an Endocrine Disorder?
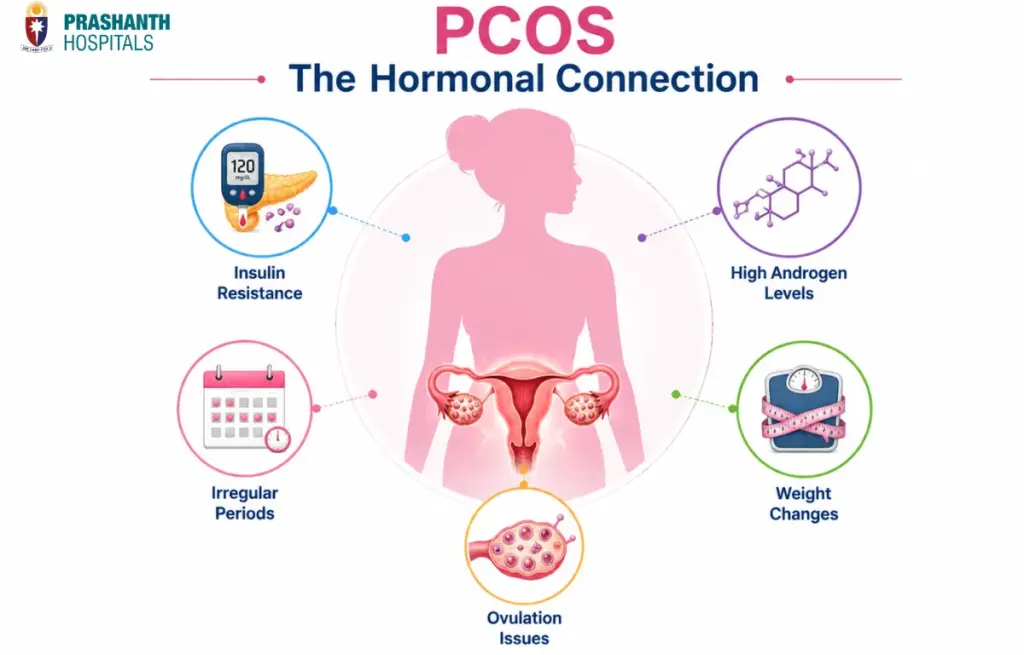
Yes. Polycystic ovary syndrome is classified as an endocrine disorder because its root cause lies in how hormones are produced and regulated, not just in the ovaries themselves.
The endocrine system is the network of glands in your body that produce hormones. Hormones are chemical messengers. They travel through the bloodstream and tell different organs and tissues what to do. The thyroid, pancreas, adrenal glands, hypothalamus, and pituitary gland are all part of this system, and so are the ovaries.
In polycystic ovary syndrome, the disruption starts high up in this hormonal chain, at the level of the hypothalamus and pituitary gland in the brain. The signal sent down to the ovaries is abnormal. The ovaries respond by producing too much of certain hormones. This sets off a cascade of effects that reaches far beyond the reproductive system alone.
Because the hormonal disruption in PCOS involves the endocrine system at multiple levels, it is managed not just by gynaecologists but also by endocrinologists, and sometimes by both working together. This is particularly true for women who also have significant insulin resistance, thyroid problems, or metabolic concerns alongside their PCOS.
The Pathogenesis of Polycystic Ovary Syndrome
Pathogenesis is a medical term that means how a condition develops step by step inside the body. Understanding the pathogenesis of polycystic ovary syndrome helps explain why it causes such a wide range of symptoms.
Here is what happens, in plain English.
Step 1: An abnormal hormonal signal from the brain.
The hypothalamus in the brain sends signals to the pituitary gland using a hormone called GnRH. In women with PCOS, these signals are sent more frequently than normal. The pituitary gland responds by releasing a hormone called LH (luteinising hormone) in higher amounts and more often than it should. FSH (follicle-stimulating hormone), which works alongside LH, does not rise proportionally. This imbalance between LH and FSH is a key feature of PCOS.
Step 2: The ovaries produce too many androgens.
LH signals the ovaries to produce androgens, which are often described as male hormones but are present in smaller amounts in all women. When LH is consistently elevated, the ovaries produce more androgens than the body needs. Testosterone is the most commonly measured androgen in PCOS. This excess is called hyperandrogenism.
Step 3: Normal egg development is disrupted.
Each month, follicles in the ovaries begin to mature in response to FSH. One follicle is supposed to become dominant, release an egg, and trigger ovulation. In polycystic ovary syndrome, the low FSH environment and the high androgen environment prevent this from happening properly. Multiple small follicles start to develop but none fully matures or releases an egg. These undeveloped follicles remain in the ovary and appear as small cysts on an ultrasound.
Step 4: Insulin resistance makes things worse.
Many women with PCOS also have insulin resistance. This means their cells do not respond properly to insulin, the hormone that controls blood sugar. To compensate, the pancreas produces more insulin. High insulin levels independently stimulate the ovaries to produce even more androgens. This creates a reinforcing cycle where high androgens and high insulin keep driving each other.
Step 5: A self-sustaining hormonal loop.
The result is a cycle where hormonal imbalance in the brain leads to excess ovarian androgens, which disrupt ovulation, which is worsened by insulin resistance, which further raises androgens. This is why the pathogenesis of polycystic ovary syndrome is considered complex and why treating only one part of the picture rarely resolves all the symptoms.
Understanding this chain of events is important because it explains why PCOS cannot simply be fixed by treating the ovaries alone. The hormonal disruption involves the brain, the pancreas, the adrenal glands, and the ovaries together.
Recognising the Symptoms of Polycystic Ovary Syndrome
Because polycystic ovary syndrome affects multiple hormone systems, its symptoms are wide-ranging. Not every woman will experience all of them. Some women have only mild symptoms. Others find that several symptoms occur together and significantly affect their daily life.
Common symptoms include:
- Irregular periods, which may come infrequently, last longer than usual, or stop altogether
- Excess hair growth on the face, chin, chest, or abdomen, known as hirsutism, caused by elevated androgens
- Hair thinning or loss on the scalp, particularly along the centre parting
- Acne, especially along the jaw and chin
- Weight gain, particularly around the abdomen
- Difficulty conceiving due to irregular or absent ovulation
- Darkening of skin in folds around the neck, armpits, or groin, a sign of insulin resistance
- Fatigue and low energy levels
- Mood changes, anxiety, and depression, which are more common in women with PCOS than in the general population
If several of these symptoms are familiar to you and you have not yet been evaluated, a conversation with your doctor is the right starting point.
Polycystic Ovary Syndrome and Electrolysis: What You Need to Know
Excess facial and body hair is one of the most distressing symptoms of polycystic ovary syndrome for many women. It is caused by elevated androgens stimulating hair follicles in areas where women do not normally grow coarse, dark hair. This includes the chin, upper lip, cheeks, chest, and abdomen.
Temporary hair removal methods like threading, waxing, shaving, and depilatory creams remove hair at the surface but do not address the follicle itself. They need to be repeated frequently and can cause skin irritation over time.
Electrolysis is a permanent hair removal method that works by passing a small electric current directly into each individual hair follicle, destroying it so that hair cannot regrow. It is currently the only method recognised internationally as providing truly permanent hair removal. It can be used on any skin tone and any hair colour, which makes it suitable for a wider range of patients than some laser-based methods.
For women with polycystic ovary syndrome, electrolysis can be an effective long-term solution for managing facial and body hair. However, there is an important consideration. If the underlying hormonal imbalance is not being treated at the same time, new hair follicles may continue to be stimulated by elevated androgens even after treated follicles have been permanently removed. This means that electrolysis works best as part of a broader management plan that includes hormonal treatment.
Laser hair removal is another option commonly used for PCOS-related hirsutism. It works faster than electrolysis for larger body areas and requires fewer sessions overall, though maintenance treatments may be needed over time. Women with darker skin tones, which is relevant for many South Indian women, should discuss appropriate laser wavelengths with their dermatologist. Not all laser systems are suitable for darker skin, and using the wrong type can cause pigmentation changes.
The most effective approach for managing polycystic ovary syndrome-related hair growth combines hormonal treatment to reduce androgen levels with a suitable hair removal method. An endocrinologist or gynaecologist can guide the hormonal side of management, while a dermatologist can advise on the best removal method based on skin tone, hair type, and the area being treated.
How Polycystic Ovary Syndrome Is Managed
Because PCOS affects multiple systems, management is usually tailored to the woman’s most pressing concerns, whether that is irregular periods, fertility, excess hair, weight, or long-term metabolic health.
Lifestyle changes come first.
In women who are overweight, losing even 5 to 10 percent of body weight can meaningfully improve hormone levels, restore more regular periods, and reduce insulin resistance. This does not require extreme dieting. Consistent, moderate changes to diet and physical activity over time produce better results than short-term approaches. A diet lower in refined carbohydrates and higher in fibre and protein tends to help manage insulin levels more effectively.
Medications to regulate periods and reduce androgens.
Combined oral contraceptive pills are frequently prescribed for women with PCOS who are not trying to conceive. They regulate the menstrual cycle and lower androgen levels, which helps with acne, hirsutism, and scalp hair thinning. Anti-androgen medications may be added in some cases to reduce excess hair growth more effectively.
Managing insulin resistance.
Metformin is an insulin-sensitising medication that is commonly used in PCOS, particularly in women with significant insulin resistance or those at higher risk of developing type 2 diabetes. It can help regulate the menstrual cycle, improve the response to fertility treatment, and reduce long-term metabolic risk.
Fertility support.
Many women with polycystic ovary syndrome go on to have successful pregnancies. For those who need help conceiving, ovulation induction is the first-line option, using medications to stimulate the ovaries to release an egg. For women who do not respond to medication, other assisted reproductive options are available. Speaking with a fertility specialist early is worthwhile so that the right plan can be put in place.
Long-term health monitoring.
Women with PCOS have a higher risk over time of developing type 2 diabetes, high blood pressure, and abnormal cholesterol levels. Regular health checks allow these to be identified and managed early.
PCOS Care at Prashanth Hospitals, Chennai
Polycystic ovary syndrome is a condition that touches many aspects of a woman’s health. Managing it well requires more than a single appointment and a single prescription. It requires a team that understands the hormonal, metabolic, reproductive, and emotional dimensions of the condition.
At Prashanth Hospitals, our Endocrinology and Obstetrics and Gynaecology departments work together to provide integrated care for women with PCOS. Whether your primary concern is irregular periods, difficulty conceiving, excess hair, weight management, or long-term metabolic health, our specialists will assess your individual situation and build a management plan that makes sense for where you are right now.
If you have been diagnosed with PCOS or are experiencing symptoms that have not yet been explained, book a consultation with our team at Prashanth Hospitals today. Getting the right diagnosis and the right support early makes a real difference to outcomes over time.